Our Health Library information does not replace the advice of a doctor. Please be advised that this information is made available to assist our patients to learn more about their health. Our providers may not see and/or treat all topics found herein.


Upper Gastrointestinal (GI) Endoscopy
Procedure Overview
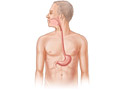
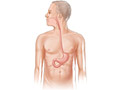
An upper gastrointestinal (GI) endoscopy is a procedure that allows your doctor to look at the inside lining of your esophagus, your stomach, and the first part of your small intestine (duodenum). A thin, flexible viewing tool called an endoscope (scope) is used. The tip of the scope is inserted through your mouth and then gently moved down your throat into the esophagus, stomach, and duodenum.
This procedure is sometimes called esophagogastroduodenoscopy (say “ih-SOF-uh-go-GAS-tro-DOO-aw-duh-NAW-skuh-pee”), or EGD.
Using the scope, your doctor can look for ulcers, inflammation, tumors, infection, or bleeding. The procedure also can be used to look for signs of acid backing up into your esophagus. This is called gastroesophageal reflux disease, or GERD. The doctor can collect tissue samples (biopsy), remove polyps, and treat bleeding through the scope. Your doctor may find problems that do not show up on X-ray tests.
Why It Is Done
An upper GI endoscopy may be done to:
- Find what's causing you to vomit blood.
- Find the cause of symptoms, such as upper belly pain or bloating, trouble swallowing (dysphagia), vomiting, or unexplained weight loss.
- Find the cause of an infection, such as Helicobacter pylori (H. pylori).
- Find problems in the upper GI tract. These problems can include:
- Inflammation of the esophagus (esophagitis) or the stomach (gastritis) or intestines (Crohn's disease).
- Gastroesophageal reflux disease (GERD).
- Celiac disease.
- A narrowing (stricture) of the esophagus.
- Enlarged and swollen veins in the esophagus or stomach. (These veins are called varices.)
- Barrett's esophagus, a condition that increases the risk for esophageal cancer.
- Hiatal hernia.
- Ulcers.
- Cancer.
- Check the healing of stomach ulcers.
- Look at the inside of the stomach and upper small intestine (duodenum) after surgery.
- Look for a blockage in the opening between the stomach and duodenum.
Endoscopy may also be done to:
- Check for an injury to the esophagus in an emergency. (For example, this may be done if the person has swallowed poison.)
- Collect tissue samples (biopsy) to be looked at in the lab.
- Remove growths (polyps) from inside the esophagus, stomach, or small intestine.
- Treat upper GI bleeding that may be causing anemia.
- Remove foreign objects that have been swallowed or food that is stuck.
- Treat a narrow area of the esophagus.
- Treat Barrett's esophagus.
How To Prepare
Procedures can be stressful. This information will help you understand what you can expect. And it will help you safely prepare for your procedure.
Preparing for the procedure
- Do not eat or drink anything for 6 to 8 hours before the procedure. An empty stomach helps your doctor see your stomach clearly during the procedure. It also reduces your chances of vomiting. If you vomit, there is a small risk that the vomit could enter your lungs. (This is called aspiration.) If the procedure is done in an emergency, a tube may be inserted through your nose or mouth to empty your stomach.
- Be sure you have someone to take you home. Anesthesia and pain medicine will make it unsafe for you to drive or get home on your own.
- Understand exactly what procedure is planned, along with the risks, benefits, and other options.
- Tell your doctor ALL the medicines, vitamins, supplements, and herbal remedies you take. Some may increase the risk of problems during your procedure. Your doctor will tell you if you should stop taking any of them before the procedure and how soon to do it.
- Remember to follow your doctor's instructions about taking or stopping medicines before the procedure. This includes over-the-counter medicines.
- If you take a medicine that prevents blood clots, your doctor may tell you to stop taking it before your procedure. Or your doctor may tell you to keep taking it. (These medicines include aspirin and other blood thinners.) Make sure that you understand exactly what your doctor wants you to do.
- Make sure your doctor and the hospital have a copy of your advance directive. If you don’t have one, you may want to prepare one. It lets others know your health care wishes. It’s a good thing to have before any type of surgery or procedure.
How It Is Done
How is an upper gastrointestinal (GI) endoscopy done?
An upper GI endoscopy may be done in a doctor's office, a clinic, or a hospital. An overnight stay in the hospital usually isn't needed.
Before the procedure
Before the procedure, you will put on a hospital gown. If you are wearing dentures, jewelry, contact lenses, or glasses, remove them. For your own comfort, empty your bladder before the procedure.
Blood tests may be done to check for a low blood count or clotting problems. Your throat may be numbed with an anesthetic spray, gargle, or lozenge. This is to relax your gag reflex and make it easier to insert the endoscope into your throat.
During the procedure
You may get a pain medicine and a sedative through an intravenous (I.V.) line in your arm or hand. These medicines reduce pain and will make you feel relaxed and drowsy during the procedure.
You will be asked to lie on your left side with your head bent slightly forward. A mouth guard may be placed in your mouth to protect your teeth from the endoscope (scope). Then the lubricated tip of the scope will be guided into your mouth. Your doctor may gently press your tongue out of the way. You may be asked to swallow to help move the tube along. The scope is no thicker than many foods you swallow. It will not cause problems with breathing.
After the scope is in your esophagus, your head will be tilted upright. This makes it easier for the scope to slide down your esophagus. During the procedure, try not to swallow unless you are asked to. Someone may remove the saliva from your mouth with a suction device. Or you can allow the saliva to drain from the side of your mouth.
Your doctor will look through an eyepiece or watch a screen while slowly moving the endoscope. The doctor will check the lining of your esophagus, stomach, and duodenum. Air or water may be injected through the scope to help clear a path for the scope or to clear its lens. Suction may be applied to remove air or secretions.
A camera attached to the scope takes pictures. The doctor may also insert tiny tools such as forceps, clips, and swabs through the scope to collect tissue samples (biopsy), remove growths, or stop bleeding.
To make it easier for your doctor to see different parts of your esophagus, stomach, and duodenum, someone may change your position or apply gentle pressure to your belly. After the exam is done, the scope is slowly pulled out.
After the procedure
You will feel groggy afterward until the medicine wears off. This usually takes a few hours. Many people report that they remember very little of the procedure because of the sedative they are given.
If your throat was numbed before the procedure, don't eat or drink until your throat is no longer numb and your gag reflex has returned to normal.
How long the procedure takes
The procedure usually takes 15 to 30 minutes. But it may take longer, depending on what is found and what is done during the procedure.
Watch
How It Feels
You may notice a brief sting or pinch when the intravenous (I.V.) needle is placed in a vein in your arm. The local anesthetic sprayed into your throat usually tastes slightly bitter. It will make your tongue and throat feel numb and swollen. Remember to relax and take slow, deep breaths.
During the endoscopy, you may feel very drowsy and relaxed from the sedative and pain medicines. You may have some gagging, nausea, bloating, or mild cramping in your belly as the tube is moved. If you have pain, alert your doctor with an agreed-upon signal or a tap on the arm. Even though you won't be able to talk during the procedure, you can still communicate.
The suction machine that's used to remove secretions may be noisy, but it doesn't cause pain. The removal of biopsy samples is also painless.
Risks
Problems, or complications, are rare. There is a slight risk that your esophagus, stomach, or upper small intestine will get a small tear in it. If this happens, you may need surgery to fix it. There is also a slight chance of infection after the procedure.
Bleeding may also happen from the endoscopy or if a tissue sample (biopsy) is taken. But the bleeding usually stops on its own without treatment. If you vomit during the procedure and some of the vomit enters your lungs, aspiration pneumonia is a possible risk.
An irregular heartbeat may happen during the procedure. But it almost always goes away on its own without treatment.
The risk of problems is higher in people who have serious heart disease. It's also higher in older adults and people who are physically weak. Talk to your doctor about your specific risks.
Results
Your doctor may be able to talk to you about some of the findings right after your endoscopy. But the medicines you get to help relax you may impair your memory, so your doctor may wait until they fully wear off. It may take 2 to 4 days for some results. Tests for certain infections may take several weeks.
Normal:
- The esophagus, stomach, and upper small intestine (duodenum) look normal.
Abnormal:
- Inflammation or irritation is found in the esophagus, stomach, or small intestine.
- Bleeding, an ulcer, a tumor, a tear, or dilated veins are found.
- A hiatal hernia is found.
- A too-narrow section (stricture) is found in the esophagus.
- A foreign object is found in the esophagus, stomach, or small intestine.
A biopsy sample may be taken to:
- Find the cause of inflammation.
- Find out if tumors or ulcers contain cancer cells.
- Identify a type of bacteria called Helicobacter pylori (H. pylori) that can cause ulcers or a fungus such as candida that sometimes causes infectious esophagitis.
Many conditions can affect the results of an endoscopy. Your doctor will discuss your results with you in relation to your symptoms and past health.
Related Information
Credits
Current as of: October 19, 2024
Author: Ignite Healthwise, LLC Staff
Clinical Review Board
All Healthwise education is reviewed by a team that includes physicians, nurses, advanced practitioners, registered dieticians, and other healthcare professionals.
Current as of: October 19, 2024
Author: Ignite Healthwise, LLC Staff
Clinical Review Board
All Healthwise education is reviewed by a team that includes physicians, nurses, advanced practitioners, registered dieticians, and other healthcare professionals.


This information does not replace the advice of a doctor. Ignite Healthwise, LLC disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use and Privacy Policy. Learn how we develop our content.
To learn more about Ignite Healthwise, LLC, visit webmdignite.com.
© 2024-2025 Ignite Healthwise, LLC.